
Introduction
General Practitioners in Brighton and Hove constitute one of the biggest interpreting service users. The wealth of experience within GP practices in using SIS community interpreters makes their feedback particularly insightful and hence valuable. In addition, access to interpreting through GPs is the best indication of language needs across the city.
As commissioners, the support of GPs for our service is increasingly important. Meeting the specific needs of both groups of customers (practitioners and service users) is a top priority for SIS; we carried out a satisfaction survey of GP surgeries in 2009 and followed up in 2011 by offering to meet with staff at GP practices to share information. Our goals were
- to gauge their views of our service delivery
- to determine priorities
- to discuss any issues or difficulties
- to gain a better understanding of the impact using SIS interpreters has
- to gather ideas about improvements or desired changes to our systems
This report brings together information from the survey and discussion groups used with data collected by SIS to explore how we can best support GP surgeries.
Statistical data
General Practitioners in Brighton and Hove usually take up approximately 22% of all interpreting sessions, making them one of the biggest users of SIS services. The uptake is spread across 44 surgeries citywide with some surgeries requiring our services on an almost daily basis.
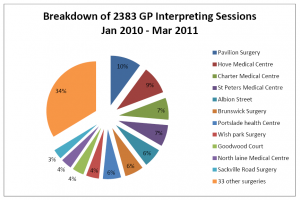
There has been an average 12% annual growth in the number of interpreting sessions required by GPs over the past 8 years. Dr Hefin Pritchard of Hove Medical Centre put this down to the changing demographic of their catchment area
“10 years ago there were very few minority ethnic individuals and communities here but now we’ve noticed it is far more diverse.” Dr Hefin Pritchard
SIS’s enhanced database provides us with an opportunity to explore the veracity of this idea, providing a breakdown for a particular practice of interpreting sessions by the number of languages and service users. This information could help surgeries adapt and tailor their services to meet the specific needs of their patients.
For Example
Hove Medical Centre needed interpreting support on 204 occasions to help 50 different patients in 7 languages. Of these, 65% were for 30 Arabic patients using on average 3 appointments per year. This indicates that Hove Medical Centre is serving a large settled community of Arabic speakers.
In contrast, Sackville Road Surgery needed interpreting support on 72 occasions to help 32 different patients in 16 languages. Of these 63% of patients had only 1 appointment in the year. This indicates that Sackville Road Surgery is serving a more transient population of isolated minority ethnic individuals.
The SIS database can also provide the GP surgery with lists of language clients who have used the service along with their appointment history. This information could be invaluable for targeting individual patients or groups for mailing translated information or other relevant services.
Satisfaction
Our 2009 survey of GP practices indicated very high levels of satisfaction with SIS on the basis of criteria suggested by the Cabinet Office Quality Mark Customer Service Excellence; information, deliver, access, timeliness and quality.
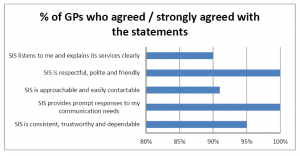
In discussions the feedback about SIS services was also overwhelmingly positive
“The service is generally very useful, the standard of interpreting is good, interpreters arrive punctually, we can book at short notice and there is rarely an unmet need.” Dr Manas Sikdar
“It’s a brilliant service. More of the same please.” Dr Andrew Mahony
Priorities
The survey also asked GPs to rank their priorities with regards to interpreting services. The top priority was the ability to book within a short period of time followed by training and continuity.
The interpreter is trained to an accredited standard
“The interpreters have a very difficult role and they need a great deal of sensitivity and delicacy particularly when they are required to intervene in order to re-focus the patient on the question or to clarify information.” Dr Andrew Mahony
There is continuity of the same interpreter
“A local interpreting service, where practitioners can build up a relationship with Community Interpreters who work with them regularly, is a massive advantage to feeling secure and trusting in their integrity to convey the messages clearly.” Dr Hefin Pritchard
Benefits
The discussion groups provided valuable insight into the main benefits of using an interpreter. Firstly, the patients can be treated effectively and a better diagnosis reached which may help prevent un-necessary return visits.
“Using an interpreter facilitates a true understanding of the case with issues explored in depth enabling patient and doctor to reach a consensus about what is going on and agree what to do. If a patient speaks a little English and no interpreter is booked we may only scratch the surface of the issue and accurate diagnosis is difficult.” Dr Susie Rockwell
Case study 1
A patient visits the surgery on a number of occasions with various different physical symptoms all of which are treated appropriately. However, it eventually becomes apparent that the physical symptoms are a result of stress which it wasn’t possible to diagnose earlier because of limitations in communication compounded by the patient’s culture which doesn’t recognise or accept psychological health issues.
Secondly, difficulties relating to the use of family members of friends can be avoided.
“There can be honest and truthful disclosure of information which may be compromised if a family member is interpreting.” Senior Nurse Cheryl Pike
Case study 2
A female patient wants to talk about Family Planning, a difficult and sensitive issue for many individuals and families. She has limited English and her husband is present and working informally as her interpreter. The practitioner gets a strong sense that the views expressed may not be those of the patient and is unsure that all the information about the various contraceptive devices is being conveyed accurately or at all.
A commitment to equal opportunities means using an interpreter is the only chance for patients with a language need to be treated fairly. However, in practice, this means that surgeries need to adapt their usual process and procedures to accommodate the specific needs of this patient group.
“Requests for Community Interpreters are patient driven. I keep up to date with patients’ level of English and whether they attend classes. On some occasions I’ve discussed these issues with patients and they have agreed they no longer need interpreting support. However, if a patient feels they need one then an interpreter will be booked.” Dr Sue Mills
Case Study 3
A patient needing an interpreter would like an urgent, same day appointment. Appointments with interpreters always take longer because everything said is repeated, therefore a double sessions is needed. There are none available so the patient is booked in to be seen at the end of surgery time. The administrative staff contact SIS to book and later confirm an interpreter. At the appointment blood tests are carried out and a further appointment with an interpreter is booked to give the results something which would usually be done over the phone.
In light of the frustrations felt in situations such as that in case study 3, we also asked whether face-to-face interpreting is still the preferred method of delivering interpreting services or whether telephone interpreting would be better. Although there was an acknowledgment that telephone interpreting may be helpful in extremely urgent scenarios, the response was a resounding negative
“Telephone interpreting wouldn’t work at all – it would be total disaster.” Dr Susie Rockwell
“Non-verbal communication is so essential and is already more difficult to gauge through an interpreter because the conversation isn’t direct but this would be so much worse if the interpreter was on the phone.” Dr Andrew Mahony
“I can’t see how it would work. General practice is about human relationships and our whole ethos centres on seeing people face to face.” Dr Sue Mills
One of the key differences between Community Interpreting and other models is that interpreters have a remit to pass on factual cultural information to Service Providers and service users alike. Whilst most GPs didn’t see this as a particular priority or benefit, Dr Nick Patton of Albion Street Surgery felt differently
“Cultural information has almost been more helpful to me than the language. In particular, cases where culturally specific body language and behaviour might be symptomatic of mental health problems.” Dr Nick Patton
Issues and Difficulties
The discussion groups identified a few concerns
- Interpreters don’t overstep their boundaries into an advocacy role
90% of all SIS interpreting sessions are carried out by accredited trained Community Interpreters and the remaining 10% by interpreters with other qualifications of relevant experience who all have a clear understanding of the differences between interpreting and advocacy. The Community Interpreters Code of Conduct gives guidance on how to remain impartial with the key tool being interpreting everything that is said during the session and only intervening for specific defined reasons.
- That patients were worried whether the stated levels of confidentiality were adhered to
It was acknowledged that SIS did everything possible to reassure patients that the sessions were completely confidential.
- That non-attendance of patients with a language need was a particular waste of time and money and whether SIS could help with this problem.
SIS has looked at this issue in detail with the PCT commissioners monitoring group and have endeavoured to generate creative ideas to solve this issue. Currently, there is no available data indicating that patients with a language need are failing to attend any more frequently than English speaking patients.
Further discussion
There were some other interesting points raised and discussions started
- the cost of interpreting
B&H City Teaching PCT has been the lead commissioner for SIS interpreting services, within a joint contract (with other NHS trusts and B&H City Council) for the past 12 years. The contract has a fixed until cost per session regardless of duration of the session and interest was expressed in the value of this for primary care.
- how a patient’s language ability (and subsequent need for an interpreter) could be objectively measured.
Ideas included the first session being conducted without an interpreter and Dr and patient would then assess whether an interpreter was needed for future appointments and/or patient can only have access to an interpreter if they are enrolled in English classes.
Conclusions
There is a great deal of satisfaction within GP practitioners about SIS services with regards delivery, quality, information provided, accessibility and timeliness. It was seen as particularly beneficial that SIS was a locally based service, offering face-to-face trained interpreters and endeavoured to provide continuity of the same interpreter for the same patient.
There were some areas identified where SIS may be able to work in close partnership with the PCT and/or individual GP surgeries to improve the delivery of services or make cost savings;
- provision of data which would help surgeries adapt and tailor their services to meet the specific needs of their patients and communities.
- facilitate the collection of feedback from patients with a language need through the National Patient Survey or other methods.
- identify creative solutions to address the issue of non-attendance at booked appointments.
- provide information for practitioners and patients about the role of interpreters, the guidelines they work to and the boundaries and limits within which they work.
- formulate strategies for empowering patients to attend without interpreters where appropriate.
Thank you
We would like to thank Dr Andrew Mahony, Dr Hefin Pritchard, Dr Sue Mills, Senior Nurse Cheryl Pike and Practice Manager Vanessa Elliot at Hove Medical Centre, Dr Nick Patton, Dr Rebecca Tillott and Dr Manas Sikdar of Albion Street Surgery and Dr Susie Rockwell of Portslade Health Centre for making timeto speak with me. Their extremely positive feedback has been most welcome and their suggestions for changes and improvements will be fully evaluated. We are looking forward to speaking to more practitioners in the future.
Vikki Gimson
Quality Assurance Manager
(revised December 2011)